Cms 1763 Form Printable
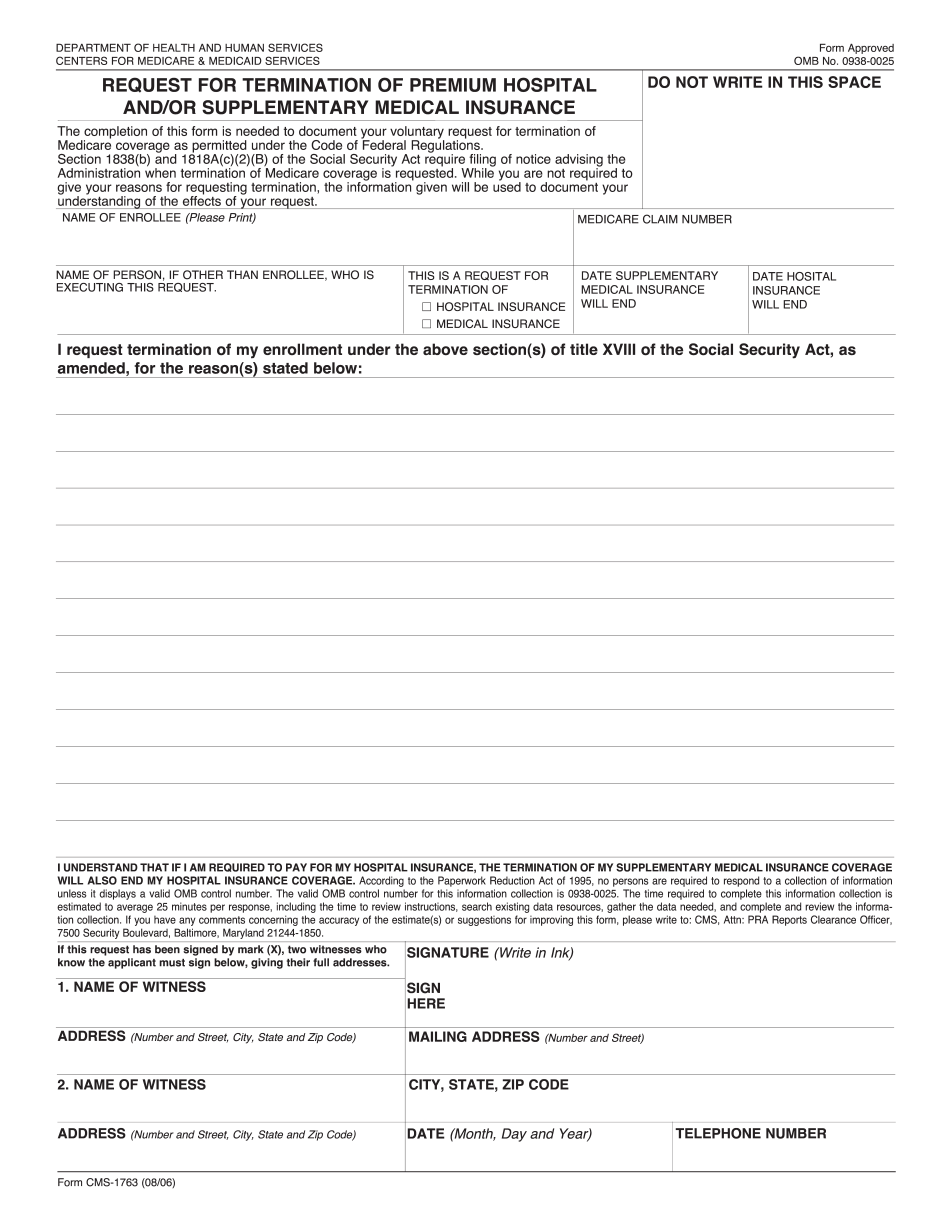
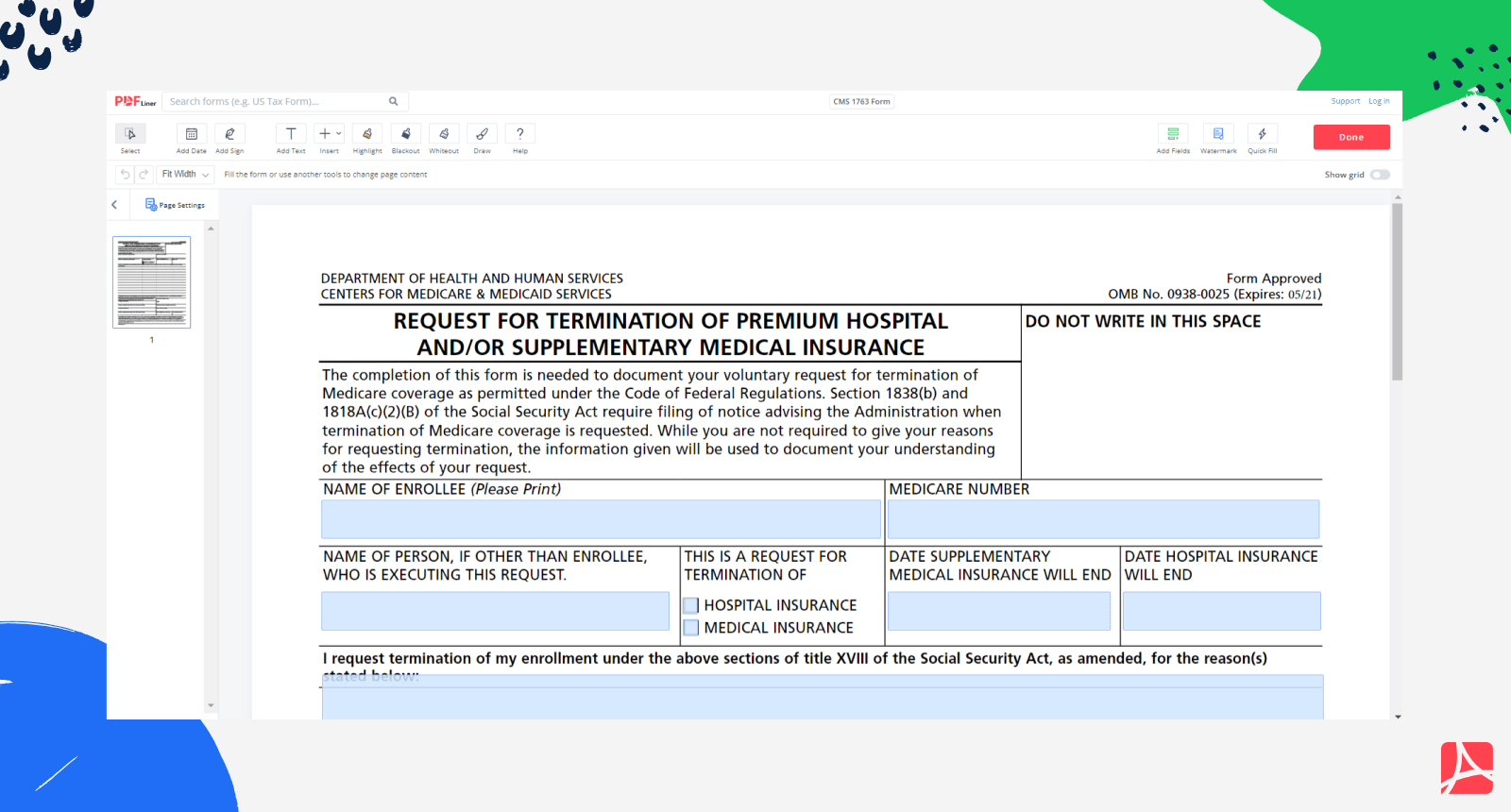
Cms 1763 Form Printable - Web this form is used for proof of group health care coverage based on current employment. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Just point and clickno downloadinstant & freepdfs made simple Request termination of my enrollment under the above sections of title xviii of the social security act, as amended, for the reason(s) stated below: How is the form completed? Section 1838(b) and 1818a(c)(2)(b) of the social security act require filing of notice advising the administration when termination of medicare coverage is requested. People with medicare premium part a or b who would like to terminate their hospital or medical. Web find the latest form for requesting termination of premium part a, part b, or part b immunosuppressive drug coverage. Department of health and human services centers for medicare & medicaid services. Other tasks you can complete at medicare.gov. The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. This information is needed to process your medicare enrollment application. Web find the latest form for requesting termination of premium part a, part b, or part b immunosuppressive drug coverage. Just point and clickno downloadinstant & freepdfs made simple. Get all forms in alternate formats. Web the cms 1763 form is a legal issued by the centers of medicare and medicaid services that allows medicare recipients to terminate their coverage of premium hospital insurance (premium part a) and/or supplemental medical insurance (part b). This is allowed under title xvii of the social security act. Web this form is used. Web first, you will need to fill out a medicare form cms 1763. Web request for termination of premium hospital. Other tasks you can complete at medicare.gov. Get all forms in alternate formats. Tbd) do not write in this space. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Web first, you will need to fill out a medicare form cms 1763. Web this form is used for proof of group health care coverage based on current employment. The centers for medicare &. Edit on any devicecancel anytimetrusted by millions30 day free trial Just point and clickno downloadinstant & freepdfs made simple Find out the consequences of disenrolling and the alternatives to save money on your premiums. This information is needed to process your medicare enrollment application. Request for termination of premium part a, part b, or part b immunosuppressive drug coverage. Web learn how to cancel your part b coverage by downloading and printing form cms 1763 and contacting the ssa. Web get forms to file a claim, set up recurring premium payments, and more. The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be conducted with everyone who. What do you use medicare form cms. Web request for termination of premium hospital. You can cancel medicare part a only if you pay a premium, and you can cancel medicare part b at any time. Request termination of my enrollment under the above sections of title xviii of the social security act, as amended, for the reason(s) stated below: Web learn how to cancel your part. However, you may need to have a personal interview with us to review the risks of dropping coverage and for assistance with your request. Web you can voluntarily terminate your medicare part b (medical insurance). Fill out the request for termination of premium part a, part b, or part b immunosuppressive drug coverage online and print it out for free.. This form is used to terminate the hospital and or medical insurance benefits you receive from medicare. People with medicare premium part a or b who would like to terminate their hospital or medical. Other tasks you can complete at medicare.gov. The centers for medicare & medicaid services (cms) requires, when possible, a personal interview be conducted with everyone who.. Web find the latest form for requesting termination of premium part a, part b, or part b immunosuppressive drug coverage. Tbd) do not write in this space. Web get forms to file a claim, set up recurring premium payments, and more. Web first, you will need to fill out a medicare form cms 1763. Find out the consequences of disenrolling. This is allowed under title xvii of the social security act. However, you may need to have a personal interview with us to review the risks of dropping coverage and for assistance with your request. People with medicare premium part a or b who would like to terminate their hospital or medical. You can cancel medicare part a only if you pay a premium, and you can cancel medicare part b at any time. Web learn how to terminate your medicare enrollment or disenrollment if you could not reach cms by phone due to challenges. Get all forms in alternate formats. Web get forms to file a claim, set up recurring premium payments, and more. Just point and clickno downloadinstant & freepdfs made simple The employer that provides the group health plan coverage completes the information about your health care coverage and dates of employment. Fill out the request for termination of premium part a, part b, or part b immunosuppressive drug coverage online and print it out for free. Web the cms 1763 form is a legal issued by the centers of medicare and medicaid services that allows medicare recipients to terminate their coverage of premium hospital insurance (premium part a) and/or supplemental medical insurance (part b). Web learn how to cancel your part b coverage by downloading and printing form cms 1763 and contacting the ssa. Web the completion of this form is needed to document your voluntary request for termination of medicare coverage as permitted under the code of federal regulations. Who can use this form? Web first, you will need to fill out a medicare form cms 1763. Other tasks you can complete at medicare.gov.
Cms 1763 Printable Form
Cms 1763 Fillable, Printable PDF Template
Cms 1763 Printable Form
Printable Form Cms 1763

Cms 1763 Printable Form Printable World Holiday
Printable Form Cms 1763
Printable Form Cms 1763
Form Cms 1763 Medicare Fill Out Online Forms Templates
Fillable Request For Termination Of Premium Hospital And/or
Form CMS1763 Download Fillable PDF or Fill Online Request for
How Is The Form Completed?
Request For Termination Of Premium Part A, Part B, Or Part B Immunosuppressive Drug Coverage.
This Form Is Used To Terminate The Hospital And Or Medical Insurance Benefits You Receive From Medicare.
Web Request For Termination Of Premium Hospital.
Related Post: